

Erectile dysfunction (ED) is a very real and debilitating disorder that affects about 22% of men between the ages of 20 and 75. With the advent of erectile dysfunction drugs like Viagra (sildenafil), Cialis (tadalafil), Levitra (vardenafil), and Spedra (avanafil), in the late 90s brought about a ‘second sexual revolution’. These drugs soared in popularity, and men everywhere realised that they were not alone in their struggle with erectile dysfunction.
In this day and age, men have more options than ever before to treat erectile dysfunction. However, the first step is the same for all treatment options: seek professional help. This is easier said than done, as one study shows that 74% of ED sufferers aged 50 and older did not discuss their sexual dysfunction issues with their doctor. While erectile dysfunction is a highly personal issue, rest assured that your doctor HAS seen and heard it all before. ED is a legitimate health condition that requires proper medical attention, and men should always consult a doctor before obtaining treatment.
The basics
What is erectile dysfunction?
Erectile dysfunction is difficulty in achieving and maintaining an erection suitable for sexual intercourse. Sometimes the penis doesn’t get hard enough, and sometimes it gets firm and softens again during penetration or before orgasm. While the reasons for this are numerous (more on that later), most men do have trouble getting or keeping an erection occasionally, particularly during times of high stress or after drinking alcohol. Infrequent difficulty in achieving or maintaining an erection should not be confused with erectile dysfunction. If these problems persist, however, a conversation with your doctor is in order.
 While incidences of erectile dysfunction do tend to increase with age, ED is not considered normal for a man of any age. Other health issues, particularly cardiovascular, can lead to erectile dysfunction. In fact, ED can actually signal to health professionals that a heart condition may be present, which makes it even more important to talk to a doctor if you are having regular difficulties with erections.
While incidences of erectile dysfunction do tend to increase with age, ED is not considered normal for a man of any age. Other health issues, particularly cardiovascular, can lead to erectile dysfunction. In fact, ED can actually signal to health professionals that a heart condition may be present, which makes it even more important to talk to a doctor if you are having regular difficulties with erections.
There are a variety of options out there for men suffering from erectile dysfunction. In addition to medications, there are vacuum devices, injections, and more simple solutions like losing weight and generally getting into better shape.
So how common is ED?
It is estimated that worldwide there will be more than 300 million sufferers of ED by 2025. In the US, according to the Massachusetts Male Ageing Study (MMAS), which followed approximately 1,700 men over a period of 17 years, 43% of the participants suffered from varying degrees of ED. This study is held in high esteem due to its longevity and attention to detail. Data collection included blood samples, health data, and biological data over three separate collection periods from 1987 to 2004.
To fully understand how and why erectile dysfunction seems to increase with age, a closer look is needed at exactly what age groups are most severely afflicted. Per the MMAS, 12% of men in the study (ages 40 to 70) suffered from complete erectile dysfunction and could never achieve and maintain an erection suitable for intercourse. The National Kidney and Urologic Diseases Information Clearinghouse breaks this down further: approximately 1% of men in their forties; 17% of men in their sixties; and 48% of men 75 and up are affected by complete erectile dysfunction.
Ageing and ED
So, if erectile dysfunction is a recognised health condition and therefore NOT simply a normal part of getting older, why the increase in incidences as men age? Certain illnesses tend to worsen as men get older and can directly affect blood flow to the penis. Erectile dysfunction may also occur as a side effect of medications used to treat these illnesses.
After retirement, many men experience drastic changes in their lifestyle. Being more sedentary, drinking more alcohol, smoking, and eating a not-so-healthy diet may be tempting after years of employment, but these factors have a negative impact on the ability to achieve and maintain an erection.
Staying healthy is the first line of defence in preventing erectile dysfunction. Surveys of healthy older couples (age 70 and up) indicate that 50-80% of couples have intercourse on a regular basis. Of those, about half reported having intercourse at least once a week. Erectile dysfunction is not inevitable as men age.
The science of an erection
Most men are familiar with the physical mechanics of an erection. Blood flows to the penis, the penis stiffens, and it softens again after orgasm is achieved. But the exact process is a bit more complicated than that.
Generally, stimulation begins in the brain, with a visual, physical, olfactory, or mental stimulus awaking the hypothalamus at the base of the brain. The brain then sends a signal down the spinal cord, signifying to the nerves in the pelvis to let blood flow into the penis.
Direct physical stimulation of the penis can also result in an erection, albeit through different nerves. The pudendal nerve brings those physical sensations from the penis to the sacral nerves in the base of the spine, which then signal to the arteries to allow blood into the penis.
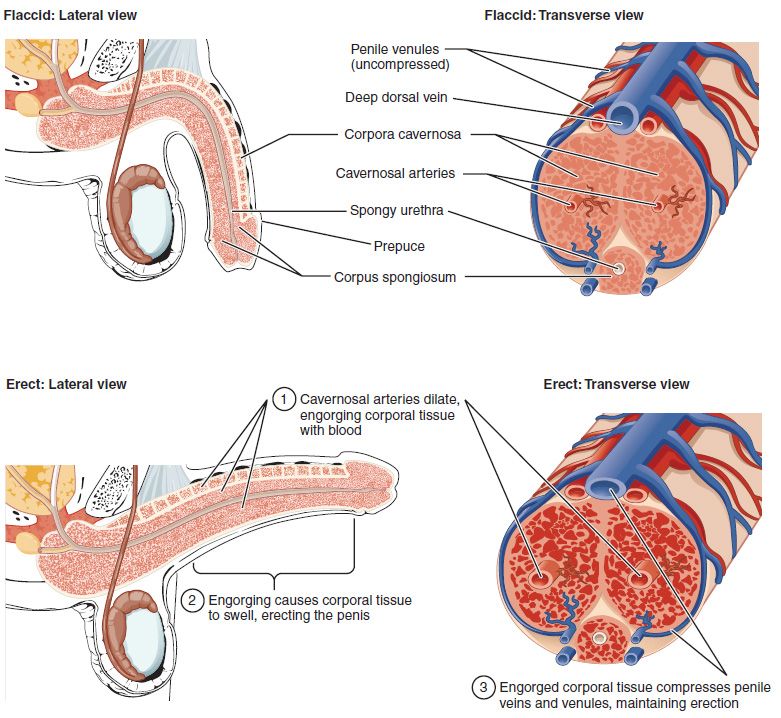
The release of nitric oxide by the nerves, in turn, stimulates the release of other chemicals that help to cause an erection. These chemicals, which include cyclic guanosine monophosphate, prostaglandins, and vasoactive intestinal polypeptide, relax the muscle cells leading to the corpora cavernosa. The corpora cavernosa are the two tubular vessels that run along the top of the penis and expand during an erection. Two main arteries run along the length of the corpora cavernosa and deliver blood to the tiny arteries that line the rest of the space. When the penis is filled with blood, the openings to the veins close up, preventing blood from draining out.
Detumescence, or the return of the penis to its flaccid state, usually occurs after orgasm. However, other factors can end an erection before orgasm is achieved. Distractions, interruptions, and low temperatures can stop the production of the chemicals responsible for erection, and phosphodiesterase 5 (PDE5) enzymes work to eliminate the remaining chemicals. Blood begins to leave the corpora cavernosa and the erection is no more.
For younger, healthy men, achieving another erection may be possible after only minutes, but for older men or those in poor health, having to wait a day or so isn’t unheard of. The amount of sexual activity a man has also impacts his ability to achieve another erection sooner rather than later. When a man goes without an erection for an extended period of time, the penis begins to lack oxygen because of the decreased blood flow. After time, muscle cells can lose their elasticity and morph into a scar tissue-like substance, which impedes the expansion of the penis.
Even with difficulty achieving erection, some men can still reach orgasm. Vice versa, some men who don’t experience erectile dysfunction have trouble climaxing. This is due to erections and orgasms being controlled by different combinations of nerves and muscles.
Even if orgasm is achieved, some men do not ejaculate. This is usually the result of taking certain medications, such as alpha blockers or selective serotonin reuptake inhibitors (SSRIs). Alpha blockers are generally used to treat conditions such as hypertension and benign prostatic hyperplasia. SSRIs are a class of antidepressants used to treat depression, anxiety, and other psychiatric issues. These types of drugs can interfere with a man’s ability to ejaculate during orgasm.
Causes of erectile dysfunction
The reasons behind erectile dysfunction are plentiful and widely varying in severity and the way they affect erections. While the previous belief was that the problem was mainly psychological, modern doctors now believe that erectile dysfunction is related to physical conditions approximately 70% of the time. But the problem isn’t restricted to one or the other.
Vascular disease
As you might expect, any illness that affects the flow of blood throughout the body is going to have an effect on erections, so it comes as no surprise that erectile dysfunction is largely caused by vascular issues. A major culprit is atherosclerosis, which is the build up of fatty deposits on the walls of the arteries. Atherosclerosis can be brought on by high blood pressure, diabetes, high cholesterol, and smoking.
A venous leak is another problem that doesn’t prevent achieving an erection, but does prevent maintaining one. Doctors aren’t certain of the cause of venous leakage, but it is clear that the blood does not remain in the penis after erection is achieved.
Abdominal aortic aneurysm is a condition in which the aorta expands, compressing the blood vessels that lead to the penis. Atherosclerosis and high blood pressure can bring on this type of aneurysm and result in erectile dysfunction.
Nerve problems
Nerve problems are most common in men who suffer from diabetes. When the nerves in or around the penis are damaged, the loss of sensation can be a factor in erectile dysfunction. Other causes of nerve damage include degenerative diseases like Parkinson’s or multiple sclerosis, substance abuse, spinal cord injury, and surgery near the affected area. A lack of vitamin B12, a main cause of anaemia, can also lead to spinal cord damage and affect the nervous system.
Diabetes
As we’ve mentioned above, diabetic nerve damage is definitely a serious problem when it comes to erectile function. Without the nerves telling the arteries to allow blood flow to the penis, the entire system of communication is shut down. Diabetes can also damage the blood vessels, leaving them unable to open up to release blood to the penis. Diabetic men also tend to have high blood pressure and cholesterol, which can also impede blood flow.
The incidence of erectile dysfunction is two to three times higher in men with diabetes than in men without. ED also tends to happen at an earlier age in men with diabetes. It starts gradually and becomes a bigger problem over time, and sometimes erectile dysfunction can be a warning sign of diabetes in men who are unaware that they have the disease.
The best way to combat diabetes-related erectile dysfunction is to gain good control over your blood sugar. Eating a healthy diet, getting enough exercise, and maintaining a healthy weight are all excellent ways to keep blood sugar levels in check. In general, men with diabetes have had success with PDE5 inhibitors like sildenafil and tadalafil.
Metabolic syndrome
Metabolic syndrome is a combination of health issues that can point to future diabetes. High triglycerides, low HDL cholesterol, hypertension, high glucose levels, and extra weight around the abdomen are all part of metabolic syndrome and can cause vascular damage and, in turn, erectile dysfunction.
Prostate cancer
Prostate cancer can contribute to erectile dysfunction both directly and indirectly. Directly, late-stage prostate cancer can spread to the nearby arteries and nerves responsible for producing an erection. Indirectly, treatment for prostate cancer can cause ED in a number of ways.
With radiation treatment, erectile tissues can be damaged. This issue happens in 38-94% of men who receive external beam radiation and in 25-50% of men who receive brachytherapy (seeds implanted in the prostate that emit radiation). It may take up to two years for erectile difficulties to show up.
Surgery to treat prostate cancer can often lead to erectile dysfunction, temporary or permanent. If nerves are severed, erectile dysfunction may very well be a permanent issue. Even without permanent nerve damage, nerve fibres may still need six to eighteen months to fully recover from the effects of surgery.
Benign prostatic hyperplasia (BPH)
BPH is a condition also known as “enlarged prostate”. The enlarged prostate itself does not cause erectile problems, but some of the medications used to treat the condition may contribute to ED. Anti-testosterone drugs like Proscar (finasteride 5mg) carry a small risk of erectile dysfunction and loss of libido. Alpha blockers also treat BPH but generally have a lower risk of causing ED. Commonly prescribed alpha blockers include Hytrin (terazosin), Flomax (tamsulosin) and Cardura (doxazosin).
On the other hand, some medications used to treat erectile dysfunction can also be used to treat BPH. Cialis (tadalafil) was approved in the US in 2001 for use in treating enlarged prostate. Five milligrams daily were sufficient to improve symptoms in men who had both BPH and ED.
TURP (transurethral resection of the prostate) is an alternative treatment for men who do not respond to medications. This surgical procedure was once thought to be connected to an increased risk for erectile dysfunction, but recent studies have shown that not only does TURP not cause ED, it can actually improve erections in some men.
Hormonal disorders
Testosterone has long been touted as the hormone that triggers sex drive and, consequently, erections. However, the link between testosterone and sexual arousal is weak. In fact, a study published by The Journal of Urology showed no connection in older men between sex hormones and their ability to achieve erections. A separate study of 1,475 men between the ages of 30 and 79 showed that only 6% of men with low testosterone levels experienced erectile dysfunction.
Though the link between testosterone and ED is uncertain, hypogonadism (the inability of the testicles to produce enough testosterone) is the leading hormonal cause of erectile dysfunction. On the other hand, men who have higher levels of luteinizing hormone (a hormone that in men boosts production of testosterone in the testes) had a lower chance of developing erectile dysfunction. Thyroid and adrenal gland issues can also contribute to ED.
Medications
Medications are responsible for approximately 25% of all cases of erectile dysfunction. Older men are more likely to take medications that list ED as a side effect. These medications include beta blockers, thiazide diuretics, and loop diuretics (all blood pressure drugs), as well as antidepressants, tranquilizers, and certain prostate drugs. Alpha blockers, ACE inhibitors, and angiotensin-receptor blockers are all medicines used to treat high blood pressure that do not usually result in erectile dysfunction. If you are on medication (prescription or over-the-counter) and are experiencing difficulty with erections, talk to your doctor about changing your dosage or switching to a different medication.
Obesity, inactivity, and poor diet
Excess weight by itself can indeed directly cause erectile dysfunction, particularly when visceral fat is present. This type of body fat surrounds the pancreas, liver, and intestines and causes some men to take on an apple-like shape. Other health issues resulting from visceral fat (such as cardiovascular disease and diabetes) can also contribute to the incidence of ED.
Even without the presence of visceral fat, being overweight is a major factor in erectile dysfunction. Research suggests that nearly 80% of men who suffer from erectile dysfunction are overweight or obese. Men with a body fat percentage of 9.8-22.6% were 21.3% more likely to have ED, while men with 30.3% body fat or higher had a 31% greater risk.
Getting enough exercise is an important part of keeping erectile dysfunction at bay. In a study of 3,941 men by the National Health and Nutrition Examination Survey at the National Institutes of Health, men who did not exercise for a minimum of 150 minutes per week had a 40-60% greater chance of developing ED. In a separate study published in the Journal of Sexual Medicine, the longer and more strenuous the exercise, the more it positively affected sexual function.
Having an unhealthy diet promotes weight gain and a host of health problems that can contribute to ED. Studies have shown that following the Mediterranean diet is linked to lower instances of erectile dysfunction and better general health overall. The Mediterranean diet consists of lots of fruits, vegetables, and whole grains, as well as protein from fish and legumes rather than red meat. Processed and refined foods are avoided, and fat comes in the form of healthy options like olive oil. This heart-healthy diet rich in omega-3 fatty acids promotes cardiovascular health and combats inflammation. The presence of flavonoids in fruits and vegetables also works to minimise the risk of ED.
More research is needed to verify this claim, but preliminary studies show that moderate caffeine intake also has a positive effect on erectile function.
Smoking
Smoking brings with it a myriad of health problems, not the least of which is erectile dysfunction. Several studies have confirmed a strong correlation between smoking and ED. In one study, smoking a pack of cigarettes per day increased the likelihood of erectile dysfunction by a whopping 60%. The study also accounted for other risk factors like blood pressure, weight, and age. Unfortunately, it seems that once the damage is done, quitting smoking does not reverse the effects of erectile dysfunction.
Alcohol and substance abuse
Drinking in moderation does not appear to be a risk factor for erectile dysfunction, and a drink or two daily may even help combat ED. Drinking heavily, on the other hand, can cause central nervous system problems, and over time, can affect the liver and cause hormonal imbalances. Illicit substances should always be avoided, as they also negatively impact the central nervous system and lead to an increase in erectile dysfunction, and can pose other health risks if used with ED medication.
Psychological factors
 The brain plays just as much a part in erections as the penis does. When a man is experiencing psychological upset, whether acute or chronic, it can affect his ability to achieve an erection. Most cases of ED have some type of psychological contributor.
The brain plays just as much a part in erections as the penis does. When a man is experiencing psychological upset, whether acute or chronic, it can affect his ability to achieve an erection. Most cases of ED have some type of psychological contributor.
When erectile dysfunction is a physical problem, the anxiety of being able to perform can negatively impact erections. This, in turn, creates a vicious cycle of worsening ED symptoms due to anxiety and higher anxiety levels because of the increase in erectile difficulties.
About 10-20% of erectile dysfunction cases are solely to blame on psychological factors. Psychogenic ED, as it is called, can be triggered by stress, anxiety, depression, guilt, or relationship problems.
In any case of ED with a psychological component, therapy can be an extremely effective tool, whether alone or with your partner. A study in 2012 separated 200 men and their partners into four groups. The men had all received either surgery or radiation as treatment for localised prostate cancer and experienced erectile dysfunction as a result. One group was put on a waiting list for therapy, two groups were assigned to online therapy, and one group was assigned to in-person therapy. After 12 weeks, the three groups that received therapy reported increased sexual function and satisfaction. The waiting list group reported no changes.
To determine whether your ED is mental or physical, your doctor will likely ask you a few questions to distinguish the cause of your erectile issues:
- Was the onset sudden or gradual? ED with a physical cause tends to be gradual, while ED with a mental cause is usually sudden.
- Do you get night time erections? Healthy men should have between three and five erections per night while sleeping. Physical causes of ED will impede nocturnal erections, while psychological causes will not.
- Does it occur with one partner or all partners? This question will not apply to everyone, but for men with multiple sexual partners, ED caused by psychological issues usually occurs with only one partner, while ED caused by a physical problem occurs with all partners.
- Does arousal occur with stimuli other than intercourse? For those with psychologically induced ED, it is possible to get an erection from other stimuli. If the ED is physical in nature, it generally is not.
Talking to your doctor and your partner is important when dealing with erectile dysfunction, especially if it is psychological in nature. Keeping the lines of communication open is crucial to treatment and recovery.
Psychological factors can also play a role in responding to treatment.
Further possible causes
Other, less common issues that can cause erectile dysfunction are as follows:
- Prostatitis – the inflammation of the prostate can directly cause ED if it is severe enough. Milder cases may make ejaculation painful, indirectly causing ED. Antibiotics may help, but allow a few weeks for your erections to return to normal.
- Peyronie’s disease – this disorder isn’t very common, but it is troublesome. Plaque accumulated in the penis hardens and causes an unnatural angle during the erection. If erections are painful or penetration isn’t possible, surgery may be able to correct the problem.
- Injury – injury to the pelvic area can cause problems when it comes to erections. Depending on the location and severity of the injury and what nerves are affected, the problem may be temporary or permanent.
- Restless legs syndrome (RLS) – RLS causes leg discomfort and the urge to move the legs, particularly during sleep. The cause of restless leg syndrome is still largely unknown, but studies have shown that sufferers of RLS are more likely to also suffer from erectile dysfunction.
- Gout – gout can indeed be an indicator of erectile dysfunction. This joint inflammation can raise the risk of ED from 51% (in men without gout) to 76% (in men with gout).
Whatever the causes of your ED, you have courses of action available to help resolve the problem. Dr Fox supplies treatment for erectile dysfunction on prescription. Answer a short medical questionnaire and choose your treatment – a prescription can be issued online and the medicine sent to your door.