
The Flaccid Truth: Erectile Dysfunction
Embed on your page - copy and paste the code below
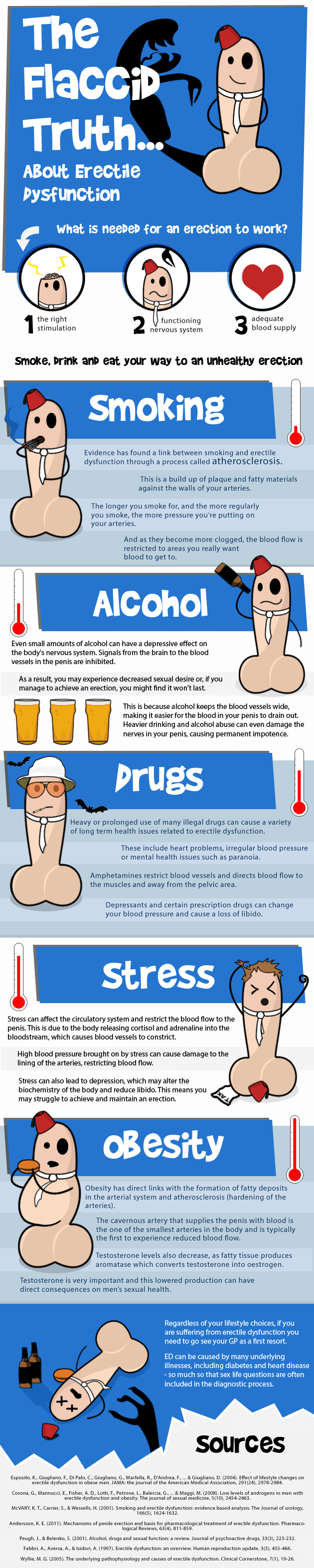
What is needed for an erection to work?
- The right stimulation
- Functioning nervous system
- Adequate blood supply
Smoke, drink and eat your way to an unhealthy erection
Smoking
Evidence has found a link between smoking and erectile dysfunction through a process called atherosclerosis.
This is a build up of plaque and fatty materials against the walls of your arteries.
The longer you smoke for, and the more regularly you smoke, the more pressure you're putting on your arteries.
And as they become more clogged, the blood flow is restricted to areas you really want blood to get to.
Alcohol
Even small amounts of alcohol can have a depressive effect on the body's nervous system. Signals from the brain to the blood vessels in the penis are inhibited.
As a result, you may experience decreased sexual desire or, if you manage to achieve an erection, you might find it won't last.
This is because alcohol keeps the blood vessels wide, making it easier for the blood in your penis to drain out. Heavier drinking and alcohol abuse can even damage the nerves in your penis, causing permanent impotence.
Drugs
Heavy or prolonged use of many illegal drugs can cause a variety of long term health issues related to erectile dysfunction.
These include heart problems, irregular blood pressure or mental health issues such as paranoia.
Amphetamines restrict blood vessels and directs blood flow to the muscles and away from the pelvic area.
Depressants and certain prescription drugs can change your blood pressure and cause a loss of libido.
Stress
Stress can affect the circulatory system and restrict the blood flow to the penis. This is due to the body releasing cortisol and adrenaline into the bloodstream, which causes blood vessels to constrict.
High blood pressure brought on by stress can cause damage to the lining of the arteries, restricting blood flow.
Stress can also lead to depression, which may alter the biochemistry of the body and reduce libido. This means you may struggle to achieve and maintain an erection.
Obesity
Obesity has direct links with the formation of fatty deposits in the arterials system and atherosclerosis (hardening of the arteries).
The cavernous artery that supplies the penis with blood is one of the smallest arteries in the body and is typically one of the first to experience reduced blood flow.
Testosterone levels also decrease, as fatty tissue produces aromatase which converts testosterone into oestrogen.
Testosterone is very important and this lowered production can have direct consequences on men's sexual health.
Lifestyle choices contributing to erectile dysfunction
Regardless of your lifestyle choices, if you are suffering from erectile dysfunction you need to go see your GP as a first resort.
ED can be caused by many underlying illnesses, including diabetes and heart disease – so much so that sex life questions are often included in the diagnostic process.
Sources
Esposito, K., Giugliano, F., Di Palo, C., Giugliano, G., Marfella, R., D'Andrea, F., … & Giugliano, D. (2004). Effect of lifestyle changes on erectile dysfunction in obese men. JAMA: the Journal of the American Medical Association, 291(24), 2978–2984. Corona, G., Mannucci, E., Fisher, A. D., Lotti, F., Petrone, L., Balercia, G., … & Maggi, M. (2008). Low levels of androgens in men with erectile dysfunction and obesity. The journal of sexual medicine, 5(10), 2454–2463. McVary, K. T., Carrier, S., & Wessells, H. (2001). Smoking and erectile dysfunction: evidence based analysis. The Journal of urology, 166(5), 1624–1632. Andersson, K. E. (2011). Mechanisms of penile erection and basis for pharmacological treatment of erectile dysfunction. Pharmacological Reviews, 63(4), 811–859. Peugh, J., & Belenko, S. (2001). Alcohol, drugs and sexual function: a review. Journal of psychoactive drugs, 33(3), 223–232. Fabbri, A., Aversa, A., & Isidori, A. (1997). Erectile dysfunction: an overview. Human reproduction update, 3(5), 455–466. Wyllie, M. G. (2005). The underlying pathophysiology and causes of erectile dysfunction. Clinical Cornerstone, 7(1), 19–26.